


Patient Centric Analytics
Many new therapies are indicated for patients with a specific disease subtype. The past 30 years of healthcare analytics have focused on targeting and segmenting physicians, facilities, and diseases. Virtually all metrics in use today aggregate activity data (e.g. total procedures) to one of the above entities. These methods were appropriate when a general description of the disease was warranted. These techniques fall short when there is a need to identify patients with a specific disease subtype.
Inflammatory Bowel Disease (IBD) Analysis
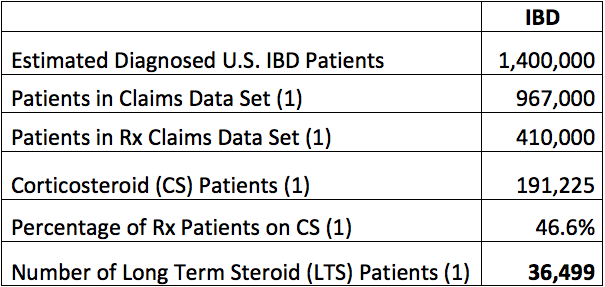
Recently we published work conducted in Inflammatory Bowel Disease[1] (IBD) that helps to demonstrate the value of Patient Centric Analysis (PCA). Short-term medium to high dose corticosteroid (CS) therapy is an effective treatment for IBD. Due to complications from long-term steroid (LTS) therapy no patients should be on medium to high dose LTS for more than 2 months continuous therapy. An analysis of claims data sets identified 36,500 LTS IBD patients in a universe of 191,225 corticosteroid IBD patients (19.1% incidence). The standard of care states that no patients with IBD should be on medium to high dose LTS. A physician or facility centric analysis would not have been able to identify these LTS IBD patients who should be evaluated for other therapies.
[1] Hommes, D. W.; Esrailian, E; Wong-Swanson, B; Centeno, A; McLaughlin, E.M.; Howard, W; Choi, J. M.; Myers, K. D.; van Oijen, M. G. Preparing for the Affordable Care Act in Inflammatory Bowel Diseases: a 2010-2012 US insurance claims analysis. Digestive Disease Week 2013.
If data are tracked and no one analyzes the information, does it make a sound???
In the last few weeks I have read numerous comments and articles that raise fair questions about the value of self-tracking or the quantified self “movement”. It reminds me a little of the early days of Microsoft and Apple arguing over which was more important, hardware or software. Self-tracking without analysis and learning from the effort is a little like buying an early PC and not buying software to run on it.
The April 1 article by Thomas Goetz in the Atlantic, “The Diabetic’s Paradox”, describes the challenges patient’s with diabetes face self-tracking their disease. He compassionately articulated the difficulties that self-monitoring causes for individuals with diabetes and quotes one study where many “regard self-monitoring as an enemy” and as a result compliance with self-tracking is low. Mr. Goetz then compares diabetes self-tracking with the new wave of self-monitoring being “recommended as a panacea” for other diseases. He asks if there are lessons to be learned from the group that has the longest track record with self-tracking. He closes with three lessons for self-tracking design by saying it should be effortless, consumer oriented, and address the emotional needs of the patient.
I agree with Mr. Goetz’s recommendations and I offer two more. Data collection without integration and analysis is futile. I echo the comments from the Strangely Diabetic Blog where Mr. Strange states, “Data by itself, with no analysis, is totally meaningless.” First, we have to find ways to make it easy for the individual to integrate information from several different sources. Then most importantly, we must give them a tool to aid in their analysis and insights. To date, little has been done to help individuals integrate and gain wisdom from their own EHR, activity, dietary, and medical self-tracked information. We have to give them meaningful and actionable insights for going through the physical and emotional hassle of collecting data.
New data and ways of capturing them are readily available. The challenge is that all of the data are in silos and cannot be easily integrated for analysis. We have to focus our efforts on ways to identify, integrate and mine disparate data sets to help individuals improve their own health. In biology there is a term called “hybrid vigor” or “heterosis” which refers to an offspring’s superior qualities or vigor that result from crossbreeding genetically diverse parents. Could it be that there might be an “Information Hybrid Vigor” or “Information Heterosis” realized by bringing together individual centric medical history, activity, and nutrition data to find successful patterns of behavior? Can we build an interpretative analysis engine that would recommend small behavior changes that would yield leveraged health benefits?
The time is now. We need to give the individual the tools to better understand where they are in their disease and deliver daily insights about small incremental changes that can be made to improve their diabetes outcomes.
Read MoreStrategy: Why Big Pharmas Do What They Do — And How Silicon Valley Might Help Them Think Differently – Forbes
See on Scoop.it – Individual Centric Healthcare

Medical product companies that figure out how to embrace and most effectively apply emerging analytic and digital health technologies, and think creatively about new risk-sharing business models, will be best positioned to deliver impactful…
Good article on Frobes.com by David Shaywitz, MD. PhD (Harvard, MIT) on the challenges BioPharma companies are facing. Of note, the "Three Alternative Approaches" does a great job summarizing the leading edge of new ways to address current challenges.
Dr. Shaywitz’s "Analytics" and "Phenotype" alternatives that are described highlight the potential value of the integration of disparate data sets and Patient Centric Analyses. The alternatives may be particularly well suited for disease categories where the ideal patient population is small. Today’s niche disease categories have created a need to identify small subsets of patients. These are individual patients who are difficult to target within a larger disease with traditional data sets. There are new patient centric analytic strategies and data sets available to meet this need.
See on www.forbes.com
Read More2012 ARM – Impact of Comparative Effectiveness Research on HSR – Training & Professional Resources – AcademyHealth
See on Scoop.it – Individual Centric Healthcare
2012 Panel on Clinical Effectiveness Research. Great quotes by Reed Tuckson, United Health Group.
"The only place that you can go anymore to get another dime (for healthcare) is on the consumer. …. The consumer is the only place you can cost shift to."
…. "Dissemination (of information) is not the problem. There are huge amounts of information with a plethora of ways to get it out. The rate limiting step is how do we educate people to make choices in an era of uncertainty. Especially in a genomics where the answers are not clear cut, but probabilistic."
See on www.academyhealth.org
Read MoreHealthcare Information Strategy & Insights
New Strategies to Better Frame Markets:
The past 30 years of Healthcare marketing analytics have focused on targeting and segmenting physicians, facilities, and diseases. Virtually all metrics in use today aggregate activity data (e.g. total procedures or total prescriptions) to one of the above entities. These methods were appropriate when a general description of the market was warranted. Identifying the key targets for a blockbuster category like dislipidemia is one example. However, as more niche markets evolve like the new class of drugs PCSK9 to treat statin resistant dislipidemia patients the old analytic techniques may fall short. The previously accepted analytic standards may actually mislead stakeholders as to where the need really is.
The addition of new robust data sets now allow the analysis to focus on patients versus providers and diseases to better frame a given market. There are HIPAA compliant strategies to integrate medical & pharmacy claims data sets with lab result, EHR and consumer demographic databases. These new data sets and methods will help better describe an addressable market based on ideal patients for a given intervention. The old provider centric approach may identify two physicians who both treat 1,000 patients. The new patient centric approach will highlight that one of those physicians has over 800 of their patients who meet the niche criteria while the other may only have 200 patients.
No one benefits from an expensive therapy being used when it is not needed. The patient centric analytics approach will have greatest leverage for more expensive niche therapies like biologics. Typically, with newer expensive therapies, the true patient population is a small subset of patients with a more severe form of the disease/condition. If your true focus is a small subset of patients who are difficult to identify within a larger disease there are new analytic techniques and data sets that can deliver vital insights. New or rarely used data sets can be brought together in interesting ways to better identify the ideal patient type via patient centric analytics.
Background:
I have over 30 years experience in Healthcare life sciences and Health Economics and Outcomes Research. My experiences range from founding Healthcare IT startups to pharmaceutical sales management, marketing, and managed care positions. I have extensive experience developing and implementing analytic solutions for payers, providers, pharmaceutical, biotech, diagnostic, and medical device organizations.
Over the past 20 years I have specialized in designing, developing, and selling Healthcare IT solutions in entrepreneurial settings. Most of the solutions focused on integrating disparate data sets in creative ways to better identify patients for targeted healthcare solutions. These solutions have a proven track record in targeting and segmenting patients and providers. Moreover, several solutions utilized Health Economics and Outcomes Research findings to improve disease outcomes and lower healthcare costs.
Read MoreAbout the Author

I focus my efforts on ways to identify, integrate and mine disparate data sets to help individuals improve their own health. Today most healthcare analysis is provider, facility, or geography centric and focuses on overall performance or practice/facility/unit variation in care. All are worthy topics, however, few seem to be focused on the individual. Can the same data sets be utilized to build an interpretative analysis engine that would recommend small behavior changes to individuals which would yield leveraged health benefits? Can we mine the currently available healthcare data to help individuals answer, "What are the small changes that I can make in my life that will have the largest impact on my overall health?" …Read More
Connect with Kelly




Recent Comments